John Michael DiBianco, Stephanie Daignault-Newton, Golena Fernandez Moncaleano, Eric Stockall, Spencer Hiller, Hyung Joon Kim, Hector Pimentel, David Wenzler, Brian Seifman, Naveen Kachroo, Casey A Dauw, Khurshid R Ghani
J Urol. 2025 Jun 9:101097JU0000000000004628. doi: 10.1097/JU.0000000000004628
Abstract
Purpose: AUA guidelines recommend ureteroscopy (URS) or shockwave lithotripsy (SWL) for lower pole (LP) stones ≤ 1 cm, while SWL is second line for stones > 1 to 2 cm. In the era of increasing URS, there are limited data on the modality used and outcomes. We assessed treatment distribution, stone-free rates (SFR), and unplanned health care.
Materials and methods: Using the Michigan Urological Surgery Improvement Collaborative registry, we identified URS and SWL cases for LP stones ≤ 2 cm (2016-2021). We assessed the frequency of patients receiving URS or SWL as a proportion of their LP treatment. A logistic model determined predictive probability of treatment modality. Differences in complete SFRs, postoperative emergency department visits, and hospitalizations were assessed by size (≤1 cm, >1-2 cm), adjusted for patient factors and correlation within practice/provider.
Results: There were 3645 procedures from 35 practices (209 surgeons); 2287 (62.7%) had SWL. 80.2% of stones were ≤ 1 cm. There was variation in modality based on practice (P < .001) and surgeon (P < .001). For stones ≤ 1 cm, the SFR was higher for URS (56% vs 39%; P < .001). There were no significant differences in SFRs for > 1 to 2 cm stones. Emergency department visits were higher after URS for stones ≤ 1 cm (OR: 2.95, 95% CI: 1.7-5.0) but not for > 1 to 2 cm stones (OR: 0.97, 95% CI: 0.4-2.2). URS for stones ≤ 1 cm was associated with increased hospitalizations (OR: 4.67, 95% CI: 1.7-12.9) but not for stones > 1 to 2 cm (OR: 0.96, 95% CI: 0.4-2.2).
Conclusions: In Michigan, SWL is the chosen modality for LP stones ≤ 2 cm. For smaller stones, URS was more effective but had greater morbidity. For larger stones, both modalities demonstrated suboptimal efficacy. Our work demonstrates the need for interventions to improve outcomes.
Comment Hans-Göran Tiselius
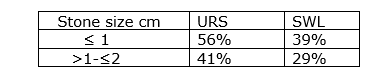
Although numerous studies have been carried out to clarify the outcome of endourology and SWL for stones located in the lower calix, the current study might be of some interest because it differentiates between smaller even 1 cm and bigger 1-smaler even 2 cm lower pole stones. There are several observations that are noteworthy. Firstly, that the selection of treatment modality differed from AUA recommendations. Secondly, for 1 cm stones URS was better than SWL. For stones bigger 1- smaller even 2 cm the methodological difference was insignificant. Thirdly, both URS and SWL offered suboptimal results, and the stone-free rates are summarized in this table:
The data reported were taken from the database MUSIC in which 209 surgeons had participated. Complications were most common in URS-treated patients.
Nothing is mentioned about facilitation of fragment elimination from the lower calyces. Given the common occurrence of residual fragments, it would be interesting to learn about the course of the disease in terms of growth, aggregation and complications over time and definitely later than the 90 days that were included in this report. It was highly interesting to find that more surgeons chose SWL before URS. Another interesting observation was that the difference between SWL and URS decreased with increasing stone size.
Despite some interesting observations in this report, it is slightly surprising that a prestigious journal like this one decided to publish these treatment results with only marginal novelty. I had expected a more sophisticated analysis of the results with more straightforward conclusions when the two treatment modalities were compared. It had indeed been interesting to learn why the results of the treatments differed and why none of the methods resulted in better stone-free rates. It is possible that anonymous databases are insufficient for necessary conclusions. In the future I wish to see summaries of detailed analyses of the treatment modalities that can move research on non/low-invasive stone removal forward. Not only to what was achieved but what in fact can be done to significantly improve the outcome. During recent years there have been too many systematic reviews, and the current reviewer would like to see more powerful efforts to improve the methods. If the basic shortcoming is residual fragments, how can we take the necessary clinical steps to improve the results?
Hans-Göran Tiselius


Although numerous studies have been carried out to clarify the outcome of endourology and SWL for stones located in the lower calix, the current study might be of some interest because it differentiates between smaller even 1 cm and bigger 1-smaler even 2 cm lower pole stones. There are several observations that are noteworthy. Firstly, that the selection of treatment modality differed from AUA recommendations. Secondly, for 1 cm stones URS was better than SWL. For stones bigger 1- smaller even 2 cm the methodological difference was insignificant. Thirdly, both URS and SWL offered suboptimal results, and the stone-free rates are summarized in this table:

The data reported were taken from the database MUSIC in which 209 surgeons had participated. Complications were most common in URS-treated patients.
Nothing is mentioned about facilitation of fragment elimination from the lower calyces. Given the common occurrence of residual fragments, it would be interesting to learn about the course of the disease in terms of growth, aggregation and complications over time and definitely later than the 90 days that were included in this report. It was highly interesting to find that more surgeons chose SWL before URS. Another interesting observation was that the difference between SWL and URS decreased with increasing stone size.
Despite some interesting observations in this report, it is slightly surprising that a prestigious journal like this one decided to publish these treatment results with only marginal novelty. I had expected a more sophisticated analysis of the results with more straightforward conclusions when the two treatment modalities were compared. It had indeed been interesting to learn why the results of the treatments differed and why none of the methods resulted in better stone-free rates. It is possible that anonymous databases are insufficient for necessary conclusions. In the future I wish to see summaries of detailed analyses of the treatment modalities that can move research on non/low-invasive stone removal forward. Not only to what was achieved but what in fact can be done to significantly improve the outcome. During recent years there have been too many systematic reviews, and the current reviewer would like to see more powerful efforts to improve the methods. If the basic shortcoming is residual fragments, how can we take the necessary clinical steps to improve the results?
Hans-Göran Tiselius