
Çavdar OF. et al., 2025: Residual stone fragments: systematic review of definitions, diagnostic standards.
O F Çavdar, A Aydin, T Tokas, A Tozsin, N Gadzhiev, M G Sönmez, R Tekeli, G Ortner, P Kallidonis, B Akgül, T Knoll, G Bianchi, J Rassweiler, K Ahmed, S Guven
World J Urol. 2025 Mar 28;43(1):194. doi: 10.1007/s00345-025-05572-x FREE PMC ARTICLE
Abstract
Purpose: Residual stone fragments (RSFs) remain a determining factor for evaluation of outcome an intervention for management of renal tract stones. However, there is a lack of consensus on size, location, diagnosis and management of RSF. This systematic review aims to assess definitions and diagnostic approaches to RSF across urolithiasis treatment modalities while standardizing their definition and diagnosis through a systematic review, stratifying RSF patients into risk groups, and proposing an approach for management.
Materials and methods: A comprehensive literature search was conducted, using Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines (PROSPERO ID: CRD42024603807). Embase, MEDLINE (PubMed) and Cochrane databases were searched until July 2024. Twentynine studies were included and categorized according to treatment choices i.e. extra-corporeal shockwave lithotripsy (ESWL) (n = 12), retrograde intrarenal surgery (RIRS) (n = 7), and percutaneous nephrolithotomy (PCNL) (n = 10). Each study's quality was evaluated using the Quadas Scoring System to determine the risk of bias and concerns regarding applicability. We included original studies that systematically defined and proposed approaches for RSF definition and diagnosis. Based on the emerging categories, we proposed a risk stratification model to classify patients accordingly.
Results: RSF definitions varied, with most studies defining RSF as fragments < 4 mm, though thresholds of < 2 mm and < 5 mm were also common. Definitions typically included only asymptomatic fragments without obstruction or infection. Computed tomography (CT) was the imaging modality most selected for diagnosis and was used in 14 studies. The timing of imaging modalities for follow-up was highly heterogeneous. The incidence of RSFs following ESWL has been reported between 21% and 59% across the studies. Among the RIRS studies, RSF rates varied between 20 and 60.5% of patients, and RSFs were observed between 20 and 60% after PCNL. The variability in RSF definitions affects comparability and may impact reintervention rates and treatment outcomes.
Conclusion: This systematic review highlights inconsistencies in defining RSFs, with common thresholds being < 2 mm, < 4 mm, or < 5 mm. CT is noted as the most reliable method for assessing fragment size and location. RSFs over 4 mm, particularly in the lower pole, are associated with higher risks of progression and complications. The review advocates to adopt standardized definitions and imaging protocols to enhance comparability and patient outcomes.
What shall we do with the residual fragments? This is a basic question that has remained ever since the introduction of non-invasive or low-invasive stone removal, but despite technical refinement of the equipment during the past four decades. The authors of this report have carried out systematic reviews with the aim of coming up with recommendations on how to deal with remaining fragments less 2 mm and up to 5 mm. Residuals most commonly reported in the literature are mentioned as less and equal 4 mm.
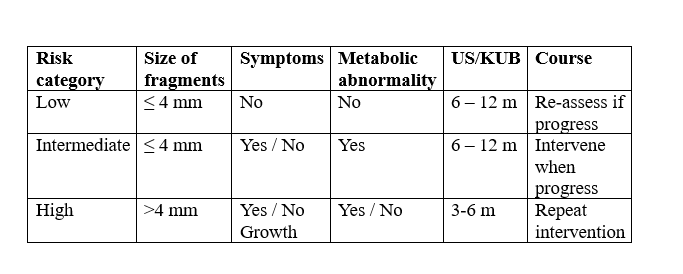
In extensive Tables this article gives detailed information on residual fragments after SWL, RIRS and PCNL The interested reader can get valuable information from these data. For readers less comfortable to read all that information, the authors have presented a clinically very useful summary in a Table. Below I present the essential recommendations.
The risk of progress and complications is highest for fragments in the lower calyx. The Table above is of value to assess the situation after stone removal because most results in the literature are expressed as stone-free ± residual fragments less and equal 4 mm.
It is important to know that residual fragments not only occur after SWL, but also follows endourological procedures. From the literature it is easy to get the impression that URS, RIRS and PCNL always leave the urinary tract without residuals. This is, however, not true.
Hans-Göran Tiselius